
“We must adapt our treatment programs to people and not people to our treatment programs.” – Dr. Eduardo Bianco
Treating Substance Use Disorders
Addiction has been recognized as a chronic brain disease since the 1990s, when the former Director of the National Institute on Drug Abuse, Dr. Alan Leshner, stated in Science that the most effective treatment and recovery options should include biological, behavioral, and social aspects. Much like other chronic diseases, including hypertension and diabetes, addiction has the potential to deeply disrupt an individual’s health and daily life and cause irreparable damage. Individuals with substance use disorders also have high rates of co-occurring disorders which include other chronic diseases and mental illnesses.
According to the National Survey on Drug Use and Health (NSDUH), in 2020, 40.3 million people aged 12 or older (or 14.5 percent) in the US had a substance use disorder in the past year. This includes 28.3 million who had alcohol use disorder, 18.4 million who had an illicit drug use disorder, and 6.5 million people who had both. Over the same period, only 4 million people (or 1.4 percent) received any sort of substance use treatment, which demonstrates the work that remains to be done (SAMHSA, 2021).
Because drug use rewards users with dopamine and teaches the brain to continue seeking dopamine at the cost of healthier activities, willpower and abstinence alone aren’t sufficient for long-term recovery. Additionally, brain imaging studies have shown that substance use and addiction alter areas of the brain that are critical for judgment, decision-making, learning, and behavior control (Shatterproof, 2022). This double-whammy of alterations in brain functioning means that most people will continue using substances despite deeply negative consequences on their health and on their lives – even after a heroin overdose.
We know of many evidence-based treatments for different forms of addiction, and highly effective medications have been developed to treat substance use disorders for alcohol, tobacco, and opioids. Medication-Assisted Treatment (MAT) within a personalized treatment plan (outpatient, inpatient, communities of care) that includes psychosocial supports (counseling, contingency management, recovery coaching, mental health services, and other services such as housing) shows overwhelmingly effective results for the treatment of opioid use disorders.
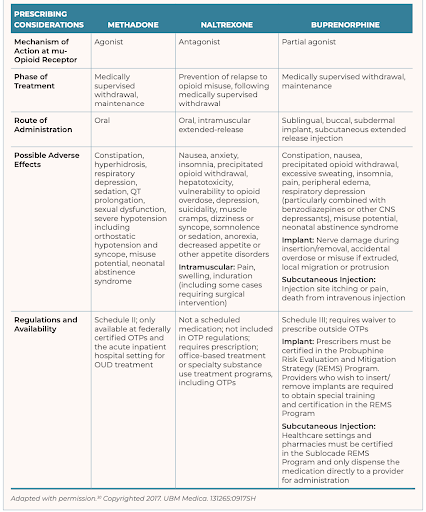
MAT has been clinically proven to reduce symptoms as well as the risk of overdose and relapse while increasing an individual’s chance of a lasting recovery (SAMHSA TIP 63). Retention in methadone and buprenorphine treatment has been shown in meta-analyses to reduce the risk of all-cause mortality and overdose mortality among people with opioid dependence by over 50% (Sordo, 2017). Research has also shown that Suboxone (a combination of buprenorphine and naltrexone) shows highly positive health outcomes, as well as Vivitrol, an injectable form of naltrexone that shows a significantly reduced risk of relapse and cravings (NIDA 2012). In addition to naloxone, a drug used to reverse overdoses, medications used to treat OUDs include methadone (an opioid agonist used to manage cravings during supervised withdrawal), naltrexone (an antagonist used to help prevent relapse after detoxification), and buprenorphine (a partial agonist used in supervised withdrawal). (Fiellin, 2008; Parran, 2010).
MAT for opioid use disorders is endorsed by the FDA, the World Health Organization, the Substance Abuse and Mental Health Services Administration, the Surgeon General, the Office of National Drug Control and Policy, the American Medical Association, the American Association of Family Physicians, and the Drug Enforcement Agency.

Lifting Barriers to Care
Until the early 2000s, we mostly relied on specialist Opioid Treatment Programs (OTP) to provide MAT services, particularly methadone, to patients. Parity laws enacted in the 1990s and reinforced with the Affordable Care Act have helped put behavioral health on par with physical health and promote integrated care as the new standard. Providers who used to operate in separate systems of primary and specialty care are now encouraged to provide mental health and substance use services in a coordinated, compassionate, and patient-centered manner, regardless of where patients might access the healthcare system.
The Drug Addiction Treatment Act of 2000 (DATA 2000) enabled physicians who fulfilled certification and education requirements to prescribe buprenorphine in primary care settings. The types of eligible providers were further expanded to include physician assistants, nurse practitioners, clinical nurse specialists, certified registered nurse anesthetists, and certified nurse-midwives. Limits on the number of patients a certified practitioner can treat each year have also been vastly increased, up to 275 patients per year. And since 2021, all physicians, nurse practitioners, physician assistants, clinical nurse specialists, certified registered nurse anesthetists, and certified nurse-midwives (totaling over 1.6 million professionals) can obtain the X-waiver allowing them to prescribe buprenorphine to up to 30 patients at a time with no certification needed – and the patient limit doesn’t apply to Emergency Departments. Gone are the days when a physician or other primary care practitioner would consider that treating substance use and addiction falls outside of their responsibilities.
The opioid crisis thrust prescription drug and heroin abuse into the spotlight. Along with facilitating treatment and recovery for addiction, there has been renewed attention and funding for primary, secondary, and tertiary prevention along the entire spectrum of substance use. Screening, Brief Intervention & Referral to Treatment (SBIRT) is an evidence-based practice that makes the assessment of substance use and its consequences a part of routine care in all healthcare settings. Healthcare practitioners (including RNs and social workers) can use brief, validated screening tools to detect use and the associated risks to the patient’s health. Based on this screening, the practitioner can then decide to conduct a brief 5-to-10-minute intervention using collaborative, motivational interviewing techniques to best engage and motivate patients to follow treatment options. For patients whose use presents higher risks, the practitioner is able to engage them in additional treatment, including a follow-up with a specialty provider, psychosocial support, medication, or inpatient treatment, depending on the level of care required. Billing codes have been approved to enable practitioners to bill public and private payers for these services.

Preparing the Workforce
Professional societies have researched and published extensive guidelines, competencies, and resources to enable workforce development on the topic of substance use. For instance, the Association for Medical Education and Research in Substance Abuse (AMERSA) has published and continuously updated extensive educational guidelines for medicine, pharmacy, nursing, social work, and physician assistants (AMERSA, 2018). In 2016, the American Board of Medical Specialties (ABMS) approved the creation of a new Addiction Medicine subspecialty, enabling physicians and osteopaths to receive a board certification in the discipline.
Governmental support for the expansion of substance use services across healthcare settings has also increased: billions of dollars have been allocated to the State Opioid Response efforts, enabling states to receive annual funding to expand treatment availability and access, particularly for the most effective evidence-based practices like MAT and naloxone. SAMHSA and HRSA also continue to fund universities, healthcare systems, and rural and community health clinics to expand workforce development efforts around MAT, SBIRT, and the integration of primary and behavioral healthcare.
Enormous barriers to care still underlie the lack of access to substance use treatment we have observed: private and public insurance still do not cover all services that are known to work; practitioner training is inconsistent, and while the American Society for Addiction Medicine has published standards of care for specialized treatment settings, there remain deep variations, and there is no nationwide certification for treatment centers.
Most of all, progress in reducing substance use and addiction continues to be hindered by deeply-entrenched stigma: the beliefs that addiction is a moral failing rather than a chronic condition, that “addicts” or “alcoholics” should be berated and lectured rather than engaged in collaborative care and shared decision-making; that harm reduction practices such as providing clean needles or Fentanyl test strips promote drug use; and that the use of medication within MAT is “just replacing one drug for another.” These baseless beliefs undermine the application of evidence-based practices to the disease of addiction and the use of medications designed to help patients enjoy a sustainable recovery and live happy, productive lives.
References
Fiellin DA, Moore BA, Sullivan LE, et al. Long-term treatment with buprenorphine/ naloxone in primary care: results at 2-5 years. American Journal of Addiction Apr 2008.
National Institute on Drug Abuse (2012). “Principals of Drug Addiction Treatment: A Research-Based Guide.” National Institute on Drug Abuse (NIDA), Dec 2012.
Parran TV, Adelman CA, Merkin B, et al. Long-term outcomes of office-based buprenorphine/naloxone maintenance therapy. Drug Alcohol Depend 1 Jan 2010.
Rutkowski, B. A. (2019). Specific disciplines addressing substance use: AMERSA in the 21st century. Substance Abuse, 40(4), 392-395.
Shatterproof. (2022) The Science of Addiction. Retrieved 5/16/22 from https://www.shatterproof.org/learn/addiction-basics/science-of-addiction
Sordo L, Barrio G, Bravo MJ, Indave BI, Degenhardt L, Wiessing L, Ferri M, Pastor-Barriuso R. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies. BMJ. 2017 Apr 26
Substance Abuse and Mental Health Services Administration. (2021). Key substance use and mental health indicators in the United States: Results from the 2020 National Survey on Drug Use and Health (HHS Publication No. PEP21-07-01-003, NSDUH Series H-56). Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/data/
Substance Abuse and Mental Health Services Administration. Medications for Opioid Use Disorder. Treatment Improvement Protocol (TIP) Series 63 Publication No. PEP21-02-01-002. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2021.
Elodie Adam
Author